Ava's Story

A Journey of Change — Navigating Anti-Racism, Empathy, and Cultural Transformation in Mental Health Care

The Awakening
Ava had been a ward manager for over a decade. She prided herself on running a fair and efficient mental health unit. Yet something had been stirring beneath the surface — a quiet discomfort she couldn’t quite name. It was in the patterns she noticed but never questioned: the disproportionate restraint of Black patients, the way certain cultural expressions were catalogued as symptoms rather than strengths.
When the invitation came for a PCREF (Patient and Carer Race Equality Framework) learning session delivered through the Phoenix Rising learning system, Ava signed up almost on impulse. She expected another compliance exercise. What she found instead was a mirror.
During the opening session, Ava was introduced to the Circle of Competence model — a framework that challenged her to recognise the boundaries of her cultural knowledge and the vast terrain of her unconscious assumptions. For the first time, she confronted a painful truth: her clinical expertise had blind spots shaped by structural racism.
“His file was thick with incident reports. But as Ava listened more carefully, she began to see something different.”
Then she met Elijah. A young Black man, 24 years old, diagnosed with schizophrenia. His file was thick with incident reports — “aggressive behaviour,” “non-compliant,” “resistant to treatment.” But as Ava listened more carefully, she began to see something different. Elijah’s animated storytelling, his spiritual references, his deep baritone voice raised in frustration — these were cultural expressions that had been misinterpreted as pathology. His “aggression” was anguish. His resistance was a survival response.
“Power is the ability to define reality and have others accept that definition as if it were their own.”— Dr. Amos Wilson
The words struck Ava with the force of revelation. She had been part of a system that defined Elijah’s reality for him — and he had never been asked to define it himself. She resolved, in that moment, to focus on what the science of empathy could teach her. The neurochemical she chose to study would change everything.
What neurochemical does Ava focus on as the key to rebuilding trust and empathy in her ward?

Echoes of History
Armed with new awareness, Ava began to dig deeper. She initiated a learning system she called “Madnificent Irations” — cultural therapy sessions that drew on the pioneering work of Professor Frederick Hickling in Jamaica. These sessions used storytelling, drama, music, and collective expression as therapeutic modalities rather than relying solely on Western clinical frameworks.
The name itself was a reclamation — “madnificent” challenging the stigma of “madness” and “irations” invoking the creative, spiritual vibrations of Caribbean culture. Patients who had been silent for months began to speak. Elijah, who had barely engaged with his care team, started singing in sessions — gospel hymns his grandmother had taught him.
Meanwhile, Ava’s research into the historical context of mental health care revealed troubling patterns. She discovered that many Victorian-era mental health institutions had been deliberately situated adjacent to prisons — a physical manifestation of the conceptual overlap between “madness” and criminality. The architecture of confinement had shaped the architecture of care.

“The architecture of confinement had shaped the architecture of care.”

“His grandfather had migrated from Jamaica in the Windrush generation. The roots of care run deeper than any single ward.”
She also encountered the concept of Drapetomania — the pseudoscientific diagnosis invented by Dr. Samuel Cartwright in 1851 to pathologise enslaved people who sought to escape captivity. Running away from slavery was classified as a mental illness. The parallel to contemporary practice was chilling: were they still, in subtle ways, pathologising resistance to oppressive conditions?
“The history of the African American people is a history of struggle against oppression.”— Dr. Joy DeGruy
Ava shared these findings with her team during a reflective practice session. The room fell silent. Some staff members shifted uncomfortably. Others nodded slowly, recognising the echoes of this history in their own ward practices. The past was not past — it was present in the policies, the language, and the power dynamics that shaped every interaction.
What was Drapetomania, and why is it relevant to modern mental health practice?

Breaking Chains
As Ava deepened her understanding of oxytocin’s role in human connection, she began to see a path forward. Oxytocin — often called the “bonding hormone” — is released during moments of genuine trust, eye contact, shared laughter, and physical comfort. It calms the amygdala, reduces cortisol, and opens neural pathways for empathy and cooperation.
Ava realised that the ward environment had been systematically suppressing oxytocin production in both patients and staff. The institutional architecture of surveillance, control, and clinical detachment created a cortisol-saturated atmosphere where threat responses dominated. Rebuilding trust would require rebuilding the neurochemical environment of care.
But change was not without resistance. During a team development session, a heated exchange brought underlying tensions to the surface. Some staff members felt personally attacked by the anti-racism focus. Others feared that acknowledging racial bias would lead to blame and punishment.
These words came from Nurse Sarah, a respected colleague who had worked on the ward for fifteen years. Her admission cracked something open in the room. It was not a confession of guilt — it was an act of courage. By naming her own bias, Sarah gave others permission to examine theirs.
“The greatest weapon against stress is our ability to choose one thought over another.”— Dr. Kenneth Hardy
Ava used this moment to introduce the concept of oxytocin-driven leadership — the idea that leaders can consciously create conditions that promote trust, belonging, and psychological safety. This was not about being “nice” — it was about understanding the neuroscience of human connection and wielding it with intention and integrity.
How does oxytocin function in building trust within clinical environments?

The Reclamation
The Madnificent Irations sessions were flourishing. What had begun as an experimental programme was now a cornerstone of the ward’s therapeutic offer. Patients from diverse backgrounds found voice through collective storytelling, drumming circles, spoken word, and dramatic re-enactment. The ward was beginning to sound different — alive with expression rather than subdued by sedation.
Ava also introduced real-time racial disparity dashboards — visual displays that tracked key metrics across ethnic groups: restraint rates, seclusion duration, medication dosages, lengths of stay, and patient satisfaction scores. The data was unflinching. Black patients were restrained at three times the rate of white patients. Their average length of stay was 40% longer. Satisfaction scores were consistently lower.
Making this data visible was an act of institutional courage. Some colleagues argued it was divisive. Ava maintained that transparency was the precondition for accountability. You cannot change what you refuse to see.
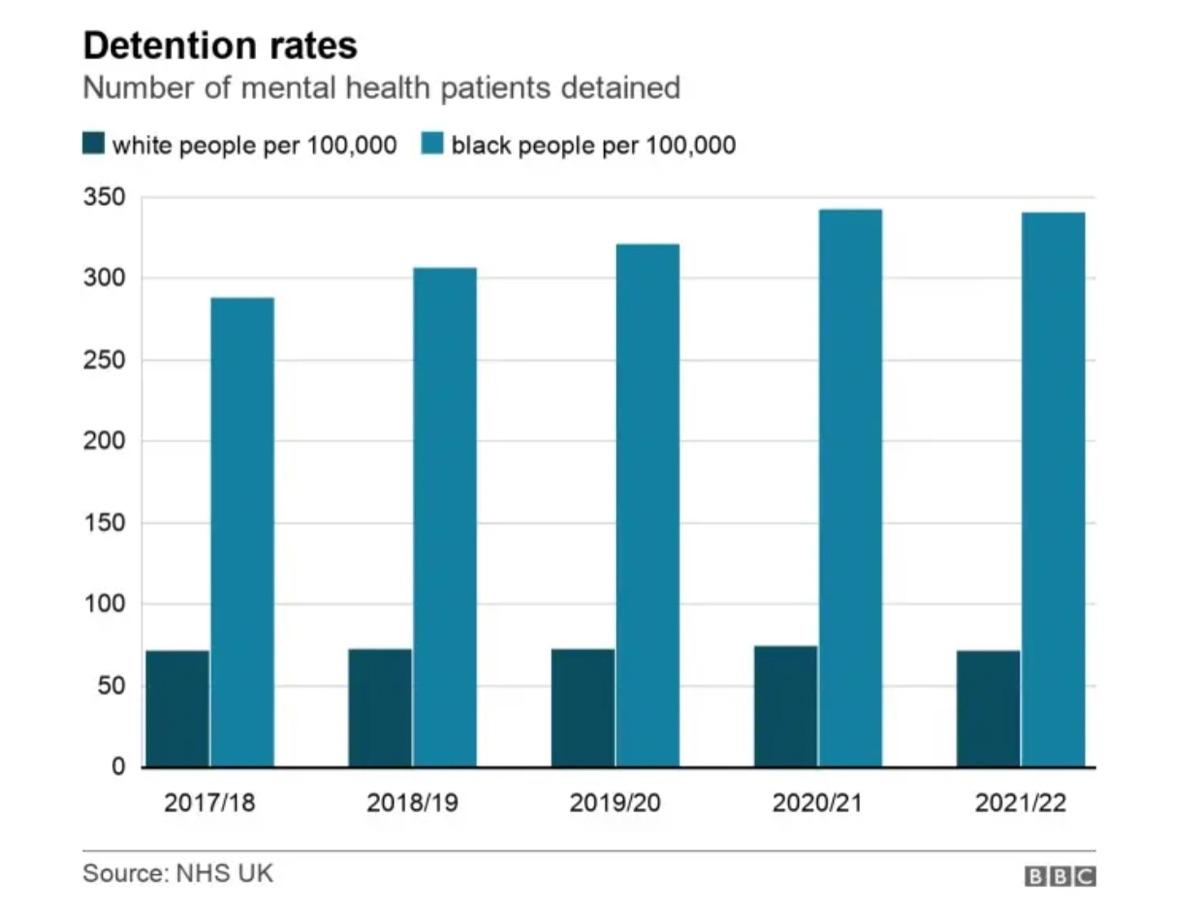
“The data was unflinching. You cannot change what you refuse to see.”
Elijah, emboldened by the storytelling sessions, began to share pieces of his family’s history. His grandfather had migrated from Jamaica in the Windrush generation. His mother had experienced postpartum depression that went undiagnosed for years because her distress was dismissed as “cultural difference.” Elijah’s own breakdown had roots in intergenerational trauma that no one had thought to explore.
Ward outcomes began to shift. Restraint incidents decreased. Staff sick leave reduced. Patient engagement scores climbed. Something was changing — not just in the numbers, but in the felt quality of care.
“We must learn to live together as brothers or perish together as fools.”— Dr. Martin Luther King Jr.
Why are racial disparity dashboards important in mental health care settings?

Threads of Change
Ava knew that cultural transformation required structural reinforcement. Compassion without systems change is sentiment. She began implementing racial equity impact assessments for every new policy, protocol, and recruitment decision on the ward. Before any change was enacted, the team asked: How might this decision affect patients and staff from different ethnic backgrounds differently?
She worked with HR to develop inclusive recruitment policies that actively sought candidates with lived experience of the communities the ward served. Interview panels were diversified. Job descriptions were rewritten to value cultural competence alongside clinical qualifications.

“These events broke down the walls between institution and community.”

“Detention rates for Black patients decreased by 20%. Something was changing.”
The results were measurable. Over the following months, detention rates for Black patients under the Mental Health Act decreased by 20%. Community engagement events brought families and local organisations into the ward for the first time. A community elder became a regular visitor, offering blessings and cultural orientation for newly admitted patients.
Ava also established community engagement events — open days where service users, families, community leaders, and faith organisations could contribute to shaping the ward’s culture. These events broke down the walls between institution and community, replacing suspicion with partnership.
“Change is never easy, but it is always possible.”— Dr. Angela Davis
Name two structural changes Ava implements to embed racial equity into ward operations.

A Vision for the Future
Elijah’s recovery was not linear — recovery never is. But through the collective healing environment that Ava and her team had created, something profound had shifted. Elijah was no longer a “difficult patient.” He was a young man with a rich cultural heritage, navigating a mental health system that was slowly learning to see him whole.
He joined the storytelling circle as a peer facilitator. He shared his grandmother’s proverbs. He taught other patients the songs that had kept his family resilient through generations of displacement. His recovery blossomed not in spite of his culture, but through it.
Ava convened a meeting of ward managers from across the trust. She shared the Phoenix Rising methodology, the data, and the stories. She invited each manager to develop their own Implementation Plan — a concrete, time-bound commitment to at least three changes they would make on their own wards.
The plans were varied and specific: one manager committed to reviewing all restraint incidents through a racial equity lens; another pledged to establish a cultural advisory board; a third planned to introduce trauma-informed communication learning for all staff. The common thread was intention — the deliberate choice to move from passive compliance to active transformation.
“The future belongs to those who prepare for it today.”— Dr. W.E.B. Du Bois

“The common thread was intention — the deliberate choice to move from passive compliance to active transformation.”
As Ava looked around the room at her colleagues — some sceptical, some inspired, all engaged — she felt the warmth of oxytocin coursing through the connections they were building. Change was not a destination. It was a practice. And the phoenix was rising.
Your Journey Begins Here
Ava’s story is a composite narrative drawn from real experiences across the UK mental health system. Her journey mirrors the transformation that the Phoenix Rising system invites you to undertake. What will your first step be?
Begin Lesson 1